What else should I write this time....
Work...nothing much bothering me since I have all my time observing and may help by giving some opinion (don't know whether it is useful or not). Feels like coming back to medical student days. Sometime I miss the role of being incharge rather than just observe other people practice. Don't worry, it will be over in a few weeks and I'm on my toes again to start my real life back. At that time may be I'll regret not to take this opportunity to appreciate this wonderful time. Thinking back... I don't even start my lecture presentation for this up coming "East coast medical update in pregnancy". I have to prepare a topic on Lupus in pregnancy...just a week after the day I'm coming back. Ok..will do it later. Typical malay..last minute job and I have 3 more weeks to think about it.
This week I've learnt more...I feel more comfortable now (I think!!) in performing ultrasound. Spend my Monday and Teusday in Xray department and used the sonographer and radiographer student as my guinea pig. They are very coorporative and allowed me to scan every single joint I wanted to. Fred at last able to use portable ultrasound from Emergency Department in POWH to teach me and we did it for an Indonesian man with extensive psoriasis with MRSA...What a patient to do scan and we need to use protective apron, that's the only suitable patient we have. Anyway, I gained information how to adjust the "pulse repetitive frequency" button to reduce excessive power doppler colour. Abbot has promised during last MSR meeting to loan some portable ultrasound to some rheumatology centres ...I think it will roughly be almost the same as what we have here. It uses a laptop as a screen and you can either use the button like in the usual u/s or you can use function as in your computer. By adjusting the image, the quality is almost as perfect as the ordinary u/s...There where you need to know a little bit back ground physic. It has only 1 level of focal zone. Wow..now I can speak the machine language better, and I can at least tell my fellow rheumato colleague...hehehe.
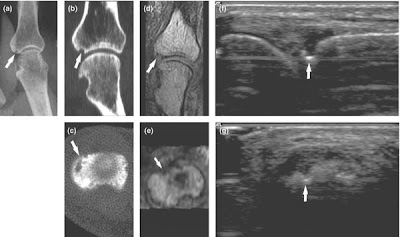
Dr Paul Bird gave me a tutorial on MRI evaluation in RA...The physic part here, frankly I can't really understand eventhough I tried hard to impress him to show I understood every aspect what he was talking about. He's a PhD qualified for MRI usage in rheumatology (Seems that if you want to have a secure position in medical field especially university setting in Australia...you need to have PhD). Pathology part seems simple after explanation...T1 image is good to look for bone erosion which appear hypointense on the bright background bone, makes MRI is such a superior tools than ultrasound to detect erosion. T2 image is good to look for oedema..in which oedematous bone will appear bright. This is useful in predicting bony erosion in RA. Having said that, it can't differentiate oedema cause by other reversible condition like trauma which may have similar appearance. T1 with fat suppression is good to look for synovitis. However, synovitis is easier detect by ultrasound rather than MRI, so most ofthe time you don't really need MRI for this. Whether joint space progression can be assess by MRI, still no definite answer as yet.This is roughly how it looks like. Google it...but image c and e is CT image.
Friday meeting as usual...great presentations. I don't know how they can get those cases. First case is a tertiary syphilis presented with lancinating type of pain over right shouder and over the subscapular region, better on shouder abduction. Presented few months before with chest pain diagnosed as having aortic disection with presence of aortic regurgitation. Pulse were equal.Imaging of shoulder and neck were normal. Inflammatory markers were normal. Evaluation for VDRL/ TPHA were positive. Interesting!! The pain most likely due lhermitte's sign. Second case is a case of DISH due to Roaccutane treatment. I've never known that...seems too many things I don't know.
Next week I've arranged my tour to Melbourne...will write my exprience later. I'm looking forward for this trip. As usual, I'll travel alone. Interesting huh!!
Work...nothing much bothering me since I have all my time observing and may help by giving some opinion (don't know whether it is useful or not). Feels like coming back to medical student days. Sometime I miss the role of being incharge rather than just observe other people practice. Don't worry, it will be over in a few weeks and I'm on my toes again to start my real life back. At that time may be I'll regret not to take this opportunity to appreciate this wonderful time. Thinking back... I don't even start my lecture presentation for this up coming "East coast medical update in pregnancy". I have to prepare a topic on Lupus in pregnancy...just a week after the day I'm coming back. Ok..will do it later. Typical malay..last minute job and I have 3 more weeks to think about it.
This week I've learnt more...I feel more comfortable now (I think!!) in performing ultrasound. Spend my Monday and Teusday in Xray department and used the sonographer and radiographer student as my guinea pig. They are very coorporative and allowed me to scan every single joint I wanted to. Fred at last able to use portable ultrasound from Emergency Department in POWH to teach me and we did it for an Indonesian man with extensive psoriasis with MRSA...What a patient to do scan and we need to use protective apron, that's the only suitable patient we have. Anyway, I gained information how to adjust the "pulse repetitive frequency" button to reduce excessive power doppler colour. Abbot has promised during last MSR meeting to loan some portable ultrasound to some rheumatology centres ...I think it will roughly be almost the same as what we have here. It uses a laptop as a screen and you can either use the button like in the usual u/s or you can use function as in your computer. By adjusting the image, the quality is almost as perfect as the ordinary u/s...There where you need to know a little bit back ground physic. It has only 1 level of focal zone. Wow..now I can speak the machine language better, and I can at least tell my fellow rheumato colleague...hehehe.
Dr Paul Bird gave me a tutorial on MRI evaluation in RA...The physic part here, frankly I can't really understand eventhough I tried hard to impress him to show I understood every aspect what he was talking about. He's a PhD qualified for MRI usage in rheumatology (Seems that if you want to have a secure position in medical field especially university setting in Australia...you need to have PhD). Pathology part seems simple after explanation...T1 image is good to look for bone erosion which appear hypointense on the bright background bone, makes MRI is such a superior tools than ultrasound to detect erosion. T2 image is good to look for oedema..in which oedematous bone will appear bright. This is useful in predicting bony erosion in RA. Having said that, it can't differentiate oedema cause by other reversible condition like trauma which may have similar appearance. T1 with fat suppression is good to look for synovitis. However, synovitis is easier detect by ultrasound rather than MRI, so most ofthe time you don't really need MRI for this. Whether joint space progression can be assess by MRI, still no definite answer as yet.This is roughly how it looks like. Google it...but image c and e is CT image.

Friday meeting as usual...great presentations. I don't know how they can get those cases. First case is a tertiary syphilis presented with lancinating type of pain over right shouder and over the subscapular region, better on shouder abduction. Presented few months before with chest pain diagnosed as having aortic disection with presence of aortic regurgitation. Pulse were equal.Imaging of shoulder and neck were normal. Inflammatory markers were normal. Evaluation for VDRL/ TPHA were positive. Interesting!! The pain most likely due lhermitte's sign. Second case is a case of DISH due to Roaccutane treatment. I've never known that...seems too many things I don't know.
Next week I've arranged my tour to Melbourne...will write my exprience later. I'm looking forward for this trip. As usual, I'll travel alone. Interesting huh!!



Ulasan